
Cancer in Medicare: An American Cancer Society Cancer Action Network Chartbook
This ACS CAN chartbook provides cancer-specific data related to Medicare, including basic information about the program, a discussion of its components, characteristics of enrollees, coverage of services – specifically those related to prevention and screening – program expenditures and enrollees’ out-of-pocket costs. This report also includes policy recommendations on how to improve the Medicare program for beneficiaries who have a history of cancer, are in active cancer treatment or who could develop cancer.
Download the Cancer in Medicare: ACS CAN Chartbook
Table of Contents
- Medicare Program Basics
- Medicare Beneficiary Characteristics
- Cancer Screening and Prevention in the Medicare Program
- Medicare Expenditures for Cancer Care
- Improvements in Medicare Still Needed
- Policy Recommendations
Introduction
The risk of cancer increases with age,i and having health insurance coverage is strongly associated with survival following a cancer diagnosis.ii Cancer is the leading cause of death among Medicare beneficiaries ages 65-74,iii and 7 out of 10 cancer deaths occur among Medicare beneficiaries.iv The Medicare program is vitally important to those who qualify including millions of older Americans and those with disabilities who are undergoing active cancer treatment, are cancer survivors or who may develop cancer. In 2024, more than 2 million Americans are projected to be diagnosed with cancer.v Over 1 million of those diagnosed are age 65 or older and rely on the Medicare program as their primary source of health care coverage.vi Cancer incidence rates also vary substantially across the U.S. (see map).
| Figure 1: Incidence Rates for United States by State, All Cancer Sites, 2016-2020 All Races (including Hispanic), Both Sexes, Ages 65+ |
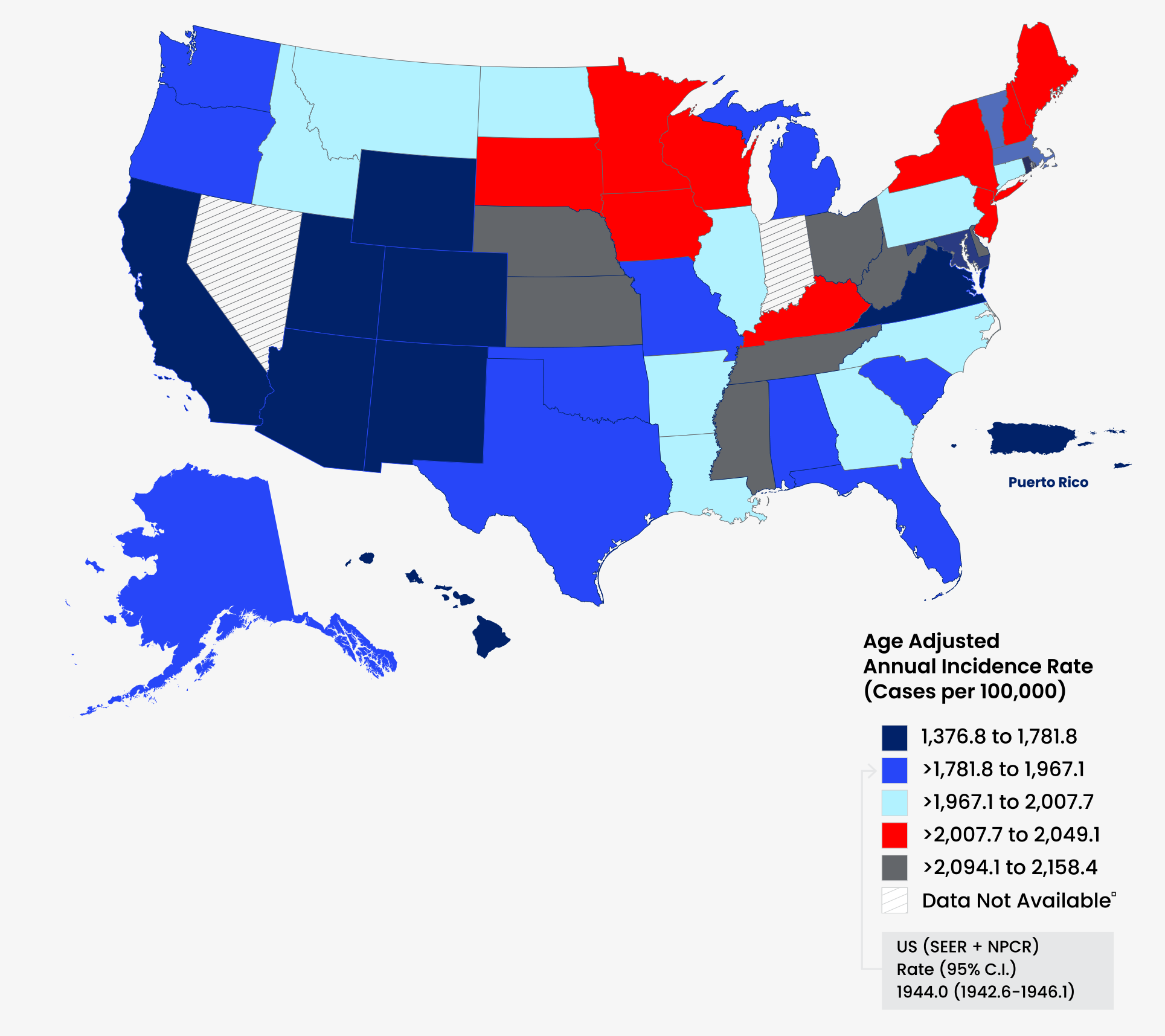 |
| Source: National Cancer Institute Cancer Profiles. Interactive Maps. 2023. Available at Interactive Maps.(cancer.gov). |
Medicare Program Basics
Medicare is a federal health program that provides health coverage for 65 million people, 57.1 million of whom qualify based on age (65 years and older) and work history (worked and paid payroll taxes for at least 40 quarters [10 years]) and 7.9 million of whom qualify based on a disability.vii Almost 9 in 10 beneficiaries are ages 65 and older, and half of beneficiaries are between the ages of 65 and 74. The total number of people enrolled in the Medicare program is expected to increase to approximately 77 million people by 2030, due in part to the baby boom generation aging into the program.viii
Components of Medicare
The Medicare program is comprised of several parts:
Medicare Part A covers inpatient hospital stays (including any cancer treatments provided as an inpatient in a hospital), skilled nursing facility stays, home health care and hospice care. Part A also covers costs of surgically implanted breast prosthesis following a mastectomy if the surgery takes place on an inpatient basis.
Medicare Part B covers physician visits, outpatient services, a limited number of preventive services, diagnostic tests, laboratory visits, durable medical equipment, some drugs (such as chemotherapy drugs administered in an outpatient clinic or physician’s office and some oral chemotherapy treatments), radiation treatments for cancer, breast prosthesis following a mastectomy if the surgery takes place in an outpatient setting and principal illness navigation services, among other services.
Medicare Part A and B are together considered to be Original Medicare (otherwise known as Original, Traditional or fee-for-service Medicare).
In Medicare Part C (also known as Medicare Advantage), beneficiaries enroll in a private health plan where they receive Part A and B benefits, usually Part D benefits and sometimes other benefits not covered under Parts A or B, such as vision and hearing services.
Part D covers outpatient prescription drugs that patients obtain at pharmacies, including some oral chemotherapy drugs, anti-nausea drugs and pain medication. The Part D program is administered through private plans contracted with Medicare.
Cancer Screening and Prevention in the Medicare Program
A significant number of cancers can be prevented. According to research from the American Cancer Society, approximately 42% of newly diagnosed cancers in the United States (about 820,000 cases in 2023) are potentially avoidable through lifestyle changes.ix Nineteen percent of all cancers are caused by smoking and 18% are caused by a combination of physical inactivity, excess body weight, poor nutrition and excess alcohol consumption.x
Importance of cancer screenings
Identifying and treating cancer at an early stage – before it has an opportunity to grow and spread and might be easier to treat – can meaningfully improve clinical outcomes. Diagnosing and treating cancer early can also reduce overall health care expenditures. In the Medicare population, average total annual costs of care are up to seven times higher for Medicare beneficiaries who are diagnosed in later stages rather than earlier stages.xi
Medicare coverage of cancer screenings
In addition to modifiable risk factors, the early detection of cancer – and in some cases, precancer – can lead to more successful treatment and increase the likelihood of survival for cancers of the breast, colorectum, cervix, lung and prostate.
Medicare Expenditures for Cancer Care
Cancer can be very expensive to treat. Given that the incidence of cancer increases with age, the costs associated with cancer treatment have a fiscal impact on the Medicare program. Over one-third (33%) of cancer costs are attributed to the Medicare population.xii Total expenditures for individuals ages 65 and older with cancer increased over the period from 2010 to 2020.
Improvements in Medicare Still Needed
The Medicare program is vitally important to ensuring that older Americans and those with certain disabilities have access to medically necessary health care services like cancer care. In fact, prior to the enactment of the Medicare program, only about half of Americans ages 65 and older had some type of coverage for hospital care, which didn’t necessarily cover surgical procedures. Since the program was enacted in 1965, it has undergone a number of major improvements, including adding the availability of coverage through Medicare Advantage plans (Part C) and coverage of outpatient prescription drugs (Part D). Unfortunately, despite these improvements, Medicare beneficiaries continue to experience barriers to accessing medically necessary care.
i American Cancer Society. Cancer Fact & Figures 2023. Atlanta: American Cancer Society; 2023.
ii Zhao, J., Han, X., Nogueira, L., Fedewa, S.A., Jemal, A., Halpern, M.T. and Yabroff, K.R. (2022), Health insurance status and cancer stage at diagnosis and survival in the United States. CA A Cancer J Clin. https://doi.org/10.3322/caac.21732.
iii Shiels MS, Haque AT, Berrington de González A, Freedman ND. Leading Causes of Death in the US During the COVID-19 Pandemic, March 2020 to October 2021. JAMA Intern Med. 2022;182(8):883–886. doi:10.1001/jamainternmed.2022.2476.
iv U.S. Cancer Statistics Working Group. U.S. Cancer Statistics Data Visualizations Tool, based on 2022 submission data (1999-2020): U.S. Department of Health and Human Services, Centers for Disease Control and Prevention and National Cancer Institute; https://www.cdc.gov/cancer/dataviz, released in June 2023.
v Cancer Facts & Figures 2024.
vi Throughout this report, we assume individuals ages 65 and older qualify for Medicare coverage. Thus, the terms Medicare beneficiary, Medicare enrollee and individuals 65+ are used interchangeably unless otherwise noted.
vii The Board of Trustees, Federal Hospital Insurance and Federal Supplementary Medical Insurance Trust Funds. 2023 Medicare Trustees Report. 2023. Available from: https://www.cms.gov/oact/tr/2023.
viii Medicare Payment Advisory Commission. A Data Book: Health Care Spending and the Medicare Program. July 2023. Available from: https://www.medpac.gov/wp-content/uploads/2023/07/July2023_MedPAC_DataBook_SEC.pdf.
ix Cancer Facts & Figures 2023. Note: This figure is for the entire population, not just the Medicare population.
x Id.
xi Reddy SR, Broder MS, Chang E, Paydar C, Chung KC, Kansal AR. Cost of cancer management by stage at diagnosis among Medicare beneficiaries. Curr Med Res Opin. 2022 Aug;38(8):1285-1294. doi: 10.1080/03007995.2022.2047536. Epub 2022 Apr 20. PMID: 35285354.
xii Ruiz ES, Seiger K, Mostaghimi A, Schmults C. National cancer expenditure analysis in the United States Medicare population, 2013. J Clin Oncol. 2019;37(15 suppl):6647. doi:10.1200/JCO.2019.37.15_SUPPL.6647.